

Around the world, many scientists are working tirelessly to find better ways to prevent and treat ovarian cancer. Dr. Omar Nelson is one of them.
Dr. Nelson and I go all the way back to our days as classmates at Titchfield High School in Jamaica. From those early beginnings, his journey has been marked by discipline, excellence, and purpose. After migrating to the United States to attend Paul Quinn College on a full Presidential Scholarship, he majored in biology with concentrations in physics, chemistry, and mathematics.
He later earned his PhD in neuroscience from University of Texas Southwestern Medical Center. Following this, he completed his postdoctoral fellowship at the University of Miami Miller School of Medicine. Although he initially focused on neurodegeneration, his research interests evolved toward gynecological cancers, specifically ovarian cancer.
Today, his research program investigates the chemopreventive effects of progestogens and vitamin D in fallopian tube–origin ovarian cancer, contributing to the growing body of work aimed at protecting and improving women’s health.
Ovarian Cancer: The Silent Disease
For many years, ovarian cancer has carried a quiet but frightening reputation. It is often called a “silent disease,” not because it lacks symptoms, but because its early signs are subtle, easily dismissed, and frequently misunderstood. By the time ovarian cancer is diagnosed, it has often progressed to an advanced stage, making treatment more complex and outcomes more uncertain. This reality has driven decades of research aimed at understanding not only how ovarian cancer grows, but where it begins.
In the past decade, scientific discoveries have challenged long-held assumptions about ovarian cancer. What was once believed to originate primarily in the ovaries is now understood, in many cases, to begin in the fallopian tubes. This shift has transformed how clinicians think about prevention, risk reduction, and early intervention. At the same time, hormones, particularly progestogens, have emerged as powerful players in understanding how risk may be lowered and, in some cases, how treatment strategies may be refined.
This evolving knowledge offers more than academic insight. It offers women clarity, empowerment, and new options for protecting their health.
The Fallopian Tubes: More Than a Pathway
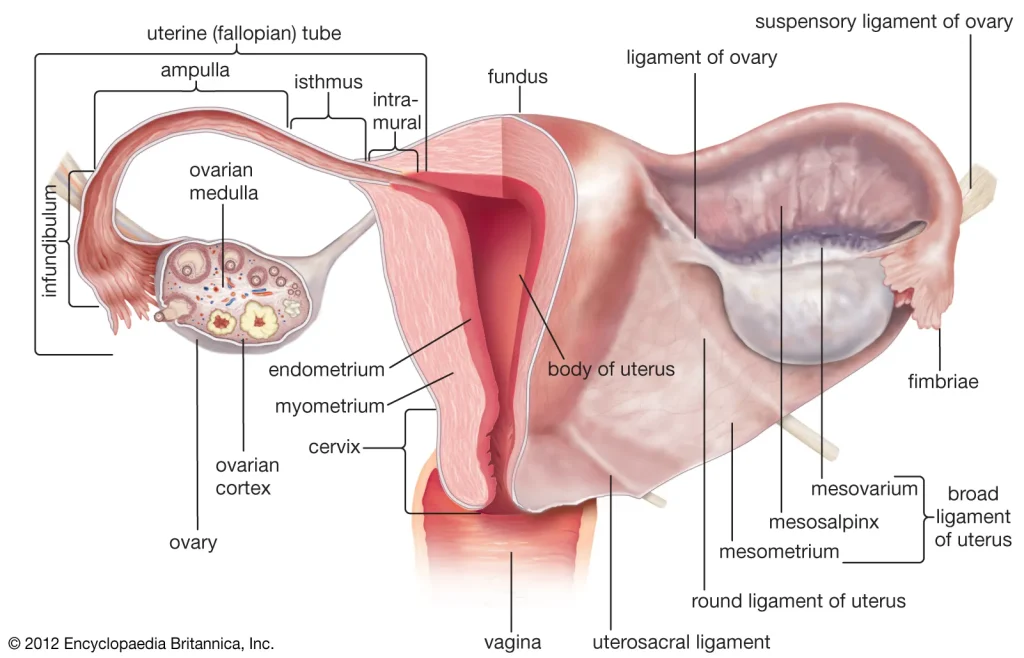
Figure 1. Showing a diagram of the uterus and fallopian tube.
For most of medical history, the fallopian tubes were viewed as simple passageways (Figure 1). Their primary role was thought to be mechanical transporting an egg from the ovary to the uterus after ovulation. While this function is essential to reproduction, research now shows that the fallopian tubes play a far more significant role in women’s health than previously understood.
Multiple studies have identified the distal end of the fallopian tube, known as the fimbriae, as the site where many aggressive ovarian cancers actually begin. Precursor lesions called serous tubal intraepithelial carcinomas, or STICs, have been found in the fallopian tubes of women with high-grade serous carcinoma, the most lethal form of ovarian cancer (Crum, C.P., 2007; Kurman, R.J., 2010). These early cellular changes can exist for years before cancer spreads to the ovaries or surrounding tissues.
This discovery has reshaped preventive care. If cancer begins in the fallopian tubes, then removing or protecting this tissue becomes a powerful strategy for reducing risk. As a result, opportunistic salpingectomy—the removal of the fallopian tubes during unrelated pelvic surgeries such as hysterectomy or sterilization—has gained support as a preventive approach (ACOG, 2019; Tone, A.A., 2019). Major medical organizations now endorse this option for women at average risk who are already undergoing pelvic surgery.
The fallopian tubes are also particularly vulnerable to damage. Chronic inflammation caused by infections, endometriosis, or repeated ovulation can injure the delicate epithelial cells lining the tubes. Over time, these injuries may accumulate genetic errors, including mutations in the p53 tumor suppressor gene, which play a central role in cancer development (Vaughan, S., 2011). This understanding has reframed the fallopian tubes as a critical focus in ovarian cancer prevention.
Ovarian Cancer: A Complex and Silent Disease
Ovarian cancer is not a single disease, but a collection of distinct tumor types with different behaviors, causes, and outcomes (Perets, R., 2016). Among these, high-grade serous carcinoma accounts for the majority of ovarian cancer deaths (Torre, L., 2018). Its aggressiveness lies not only in how quickly it grows, but also in how quietly it develops.
Early symptoms of ovarian cancer are often vague. Women may experience bloating, abdominal discomfort, changes in appetite, or urinary urgency. These signs are easily mistaken for digestive issues, stress, or normal hormonal changes. As a result, many women delay seeking care, and clinicians may not immediately suspect cancer.
Standard treatment for ovarian cancer typically involves a combination of surgery and chemotherapy. Cytoreductive surgery aims to remove as much tumor tissue as possible, followed by platinum-based chemotherapy agents such as carboplatin and paclitaxel. In recent years, targeted therapies like PARP( poly (ADP-ribose) polymerase) inhibitors have improved outcomes for certain patients, particularly those with BRCA mutations or defects in DNA repair pathways (Norquist, B.M., 2021; NCCN, 2024).
Despite these advances, recurrence remains common (Vaughan, S., 2011). This reality underscores the importance of prevention, early detection, and a deeper understanding of the biological processes that drive the disease.
Risk Factors: Genetics, Hormones, and Reproductive History
Ovarian cancer risk is shaped by a complex interplay of genetics, hormones, and life experiences. Among all known risk factors, inherited genetic mutations carry the strongest influence. Mutations in BRCA1 and BRCA2 significantly increase lifetime risk, with BRCA1 carriers facing up to a 45 percent risk and BRCA2 carriers facing up to 25 percent (Norquist, B.M., 2021). Lynch syndrome, another inherited condition, also raises risk.
Hormonal and reproductive factors play a powerful role as well. Women who begin menstruating early or reach menopause later experience more lifetime ovulations, which is associated with increased risk. Each ovulation triggers inflammation and tissue repair, creating opportunities for DNA damage over time.
Pregnancy and breastfeeding, on the other hand, reduce ovarian cancer risk. These states suppress ovulation and expose reproductive tissues to higher levels of progesterone, which appears to have protective effects. Similarly, long-term use of combined oral contraceptives has been shown to significantly lower ovarian cancer risk, an effect supported by decades of epidemiological data (Collaborative Group, 2012; Havrilesky, L.J., 2013).
Lifestyle factors such as obesity and smoking may also influence risk, although their effects vary by cancer subtype and are generally less impactful than genetic and reproductive factors.
The Role of Progestogens: Protection and Therapeutic Potential
Progestogens, which include natural progesterone and synthetic progestins, play a central role in reproductive health. Beyond regulating the menstrual cycle and supporting pregnancy, these hormones appear to influence cancer risk at the cellular level.
One leading theory suggests that progestogens promote apoptosis, or programmed cell death, in damaged or abnormal epithelial cells within the ovary and fallopian tubes (Modugno, F., 2012). This process helps eliminate cells that might otherwise accumulate mutations and become cancerous. This mechanism may explain why hormonal contraceptives containing progestins provide such strong protection against ovarian cancer (Havrilesky, L.J., 2013).
Pregnancy offers further evidence of progesterone’s protective role. During pregnancy, progesterone levels remain elevated for extended periods, potentially clearing damaged cells from reproductive tissues. Studies also show that progestin-only contraceptives, such as injectable medroxyprogesterone acetate, are associated with reduced ovarian cancer risk.
Because many ovarian cancers originate in the fallopian tubes, the responsiveness of tubal epithelial cells to progesterone signaling has become an important area of research (Tone, A.A., 2019). Progestogens may enhance cellular turnover in the tubes, reducing the likelihood that precancerous lesions will persist.
In treatment, however, the role of progestogens is more limited. While hormonal therapy is effective for some gynecologic cancers, high-grade serous ovarian cancer typically lacks the hormone receptors needed to respond (Modugno, F., 2012). Certain low-grade or hormone-sensitive ovarian tumors may benefit from hormonal approaches, but further research is needed.
Women’s Health: Early Detection and Proactive Care
Improving ovarian cancer outcomes requires more than better treatments. It demands a proactive approach to women’s health that emphasizes awareness, prevention, and informed decision-making.
Routine gynecologic care remains essential, even though no screening test has proven effective for the general population (NCCN, 2024). Regular visits allow clinicians to monitor changes, address symptoms, and assess individual risk factors. Women should be encouraged to trust their instincts and seek evaluation when symptoms persist.
Awareness of early symptoms is particularly important. Persistent bloating, pelvic pressure, difficulty eating, or urinary changes should never be ignored. While these symptoms are common and often benign, their persistence warrants medical attention.
Genetic counseling plays a vital role for women with a family history of cancer. Identifying inherited risk allows for personalized prevention strategies, including enhanced surveillance, hormonal interventions, or preventive surgery (Rebbeck, T.R., 2009).
Risk-Reducing Surgery and the Shift in Prevention
The recognition of the fallopian tubes as a primary origin site for ovarian cancer has transformed surgical prevention strategies. Opportunistic salpingectomy is now widely recommended for women undergoing pelvic surgery for other reasons, as it removes tissue most likely to develop cancer while preserving ovarian function (ACOG, 2019).
For women at high genetic risk, risk-reducing salpingo-oophorectomy remains the most effective option. However, newer approaches, such as removing the fallopian tubes first and delaying ovary removal until closer to menopause, aim to balance cancer prevention with hormonal health and quality of life (Rebbeck, T.R., 2009).
These evolving strategies reflect a more nuanced understanding of women’s bodies and the importance of individualized care.
Looking Forward: Research, Knowledge, and Empowerment
The future of ovarian cancer prevention lies in integration, combining molecular research, hormonal science, genetic testing, and patient education. Understanding the fallopian tube’s role has opened new doors for early intervention, while insights into progestogen biology offer promising avenues for risk reduction (Perets, R., 2016).
Most importantly, empowering women with knowledge transforms outcomes. When women understand their bodies, their risks, and their options, they can make informed decisions rooted in confidence rather than fear.
The story of ovarian cancer is still being written. But with continued research, proactive care, and a commitment to women’s health, the narrative is shifting, from silence and late detection to awareness, prevention, and hope.
References
- Kurman RJ, Shih I-M. The Origin and Pathogenesis of Epithelial Ovarian Cancer. Am J Surg Pathol. 2010.
- Crum CP et al. The Tubal Fimbria as Origin for Pelvic Serous Cancer. Clin Med Res. 2007.
- Perets R, Drapkin R. New Insights in Ovarian Cancer Research. Cancer Res. 2016.
- ACOG. Opportunistic Salpingectomy for Prevention. Committee Opinion No. 774. 2019.
- Vaughan S et al. Rethinking Ovarian Carcinogenesis. Nat Rev Cancer. 2011.
- Havrilesky LJ et al. Oral Contraceptives and Ovarian Cancer Prevention. Evidence Report. 2013.
- Collaborative Group on Epidemiological Studies of Ovarian Cancer. OCs and Cancer Risk. Lancet. 2012.
- Tone AA et al. The Fallopian Tube in Ovarian Cancer Prevention. J Obstet Gynaecol Can. 2019.
- NCCN Clinical Practice Guidelines: Ovarian Cancer. 2024.
- Torre LA et al. Ovarian Cancer Statistics. CA Cancer J Clin. 2018.
- Norquist BM et al. HRD and Outcomes in Ovarian Cancer. J Clin Oncol. 2021.
- Modugno F et al. Hormone Response in Ovarian Cancer. Gynecol Oncol. 2012.
- Rebbeck TR et al. Risk Reduction from Salpingo-Oophorectomy. J Clin Oncol. 2009.
About the Author
Dr. Omar Nelson is the researcher behind this story. Although he earned his PhD in neuroscience, his work now focuses on ovarian cancer and advancing prevention strategies that protect women’s health.
He currently serves as a Research Scientist at Endeavor Health and as a Research Assistant Professor at the University of Chicago Pritzker School of Medicine.
Beyond the lab, Omar is passionate about cycling and hosts the Chicago Cycling Network podcast on YouTube, where he shares his enthusiasm for the sport and community. Above all, he is a devoted husband and father.